AI for Community Health Workers in India: A Bottom-Up Approach to Technology Development (Part 3)
This is the third blog post in a three-part series exploring the development and deployment of large language models for community health workers in low-resource settings published on Open research gateway.
The George Institute for Global Health and the University of Oxford have developed SMARThealth Pregnancy 2 (SHP2), a cost-effective, app-based tablet technology. It has the potential to assist ASHAs (Accredited Social Health Activists) to identify and manage high-risk conditions throughout pregnancy and postpartum, extending up to the first year after birth. It supports community health workers, also known as ASHAs in India, in conducting home visits for screening, managing and referring women to primary and secondary health services. This system screens for high-risk conditions such as anaemia, hypertension, and gestational diabetes mellitus. It is being piloted in the rural districts of two Indian states: Haryana and Telangana.
As part of the BMGF Grand Challenges, we further developed and integrated the LLM chatbot, SMARThealth GPT, within the SMARThealth Pregnancy platform to provide real-time support and assistance to ASHA workers in delivering healthcare services to pregnant and postpartum women. We co-developed the SMARThealth GPT chatbot with the local stakeholders and made it available in two regional languages, Telugu and Hindi. The research process included iterative feedback from both ASHAs and doctors on the content, format, feasibility, and acceptability.
This photo essay will present visual glimpses of our journey and community engagement in developing SMARThealth GPT. It will feature our interactions with ASHA workers in Rohtak and Jhajjar districts of Haryana and Siddipet district of Telangana.
The following selected photos and their brief backgrounds provide a few glimpses into our journey.

The ASHA workers’ SHP scheduled visits to the women are two antenatal visits and five postpartum visits, during which they assess, screen, counsel, and appropriately refer women. Caught in this photo is one such visit of the ASHA worker. Although the SMARThealth Pregnancy 2 system is receiving positive reviews from the stakeholders1 , qualitative work found that ASHAs could benefit from additional evidence-based support, particularly continuous training and supervision for the ASHAs. A digital support system that could give ASHAs access to comprehensible guideline-based knowledge as they are faced with various maternal health questions by women in their communities, could boost the ASHAs confidence while conducting their visits for screening and assessment.

Our research team used introductory videos in their local language to introduce the ASHA workers in the SMARThealth Pregnancy trial to the concept of AI. The video demonstrated prototype of a simple chatbot using natural language processing. It ended with the prompt, “If you could ask any question related to your work, what would you want to ask this chatbot?” Our research team ran three focus groups across Haryana and Telangana to understand these future users' ‘real-world’ requirements.

Based on our past focus groups with the ASHA workers, we had pre-identified topic areas that could be important for them. We wrote 130 questions based on these topic areas. Next, we wanted to verify whether these questions were relevant to them and, if so, what the ASHA’s priority areas were. We conducted ‘pile sorting’ sessions, including 16 ASHAs as participants and divided them into four groups of 4. We then asked the participants to reflect on these questions and consider which ones are important. This pile sorting was conducted twice in Jhajjar and Rohtak districts in Haryana, and once in Siddipet district in Telangana.

The ‘pile sorting’ activity was a hit! We saw the excitement rise in the groups as they collectively decided which questions would be most relevant to them if we designed a chatbot to address their needs. Each group of ASHA workers came to a unanimous decision and placed each question in one of three piles: “frequently asked”, “sometimes asked”, and “never asked”. This helped us take a meaningful bottom-up approach as we worked our way back to add training data to the model to help address questions most frequently received by ASHAs in the field.

The excitement and positivity of the ASHA workers in understanding our development objectives proved highly beneficial to the process. As we worked through the challenges of identifying, sorting, and documenting the most frequently asked and relevant questions, our understanding of ASHAs' use of technology in their daily lives was clarified. We found that younger ASHAs were keener on adapting new technology than older ASHAs2. In the subsequent phases, we involved doctors to validate the questions and help us curate appropriate responses for the ASHA workers. The clinicians ensured that the responses were high-quality and contextually relevant, considering that ASHA workers are not medical experts.
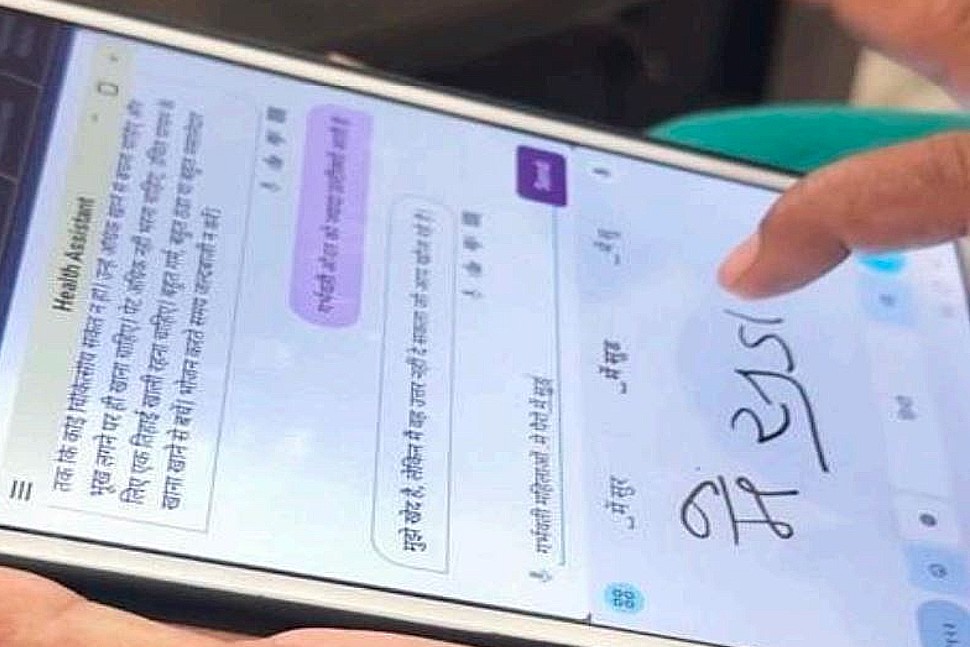
We worked with the ASHA workers to determine if the chatbot would be easy to use. To enhance its usability, we enabled audio questions and handwriting-to-text features. The photo captures one such instance during our evaluation process. The majority of ASHAs expressed a preference for the chatbot's audio questions feature and the ‘speak-out-loud' accessibility feature.
ASHA workers, being the first point of contact with the communities, have a deeper understanding of the challenges and needs of communities. Employing a bottom-up approach made the SMARThealth GPT chatbot culturally relevant and well-suited for use by the ASHA workers. Co development was crucial to identify real problems and needs and develop an appropriate technological solution which addresses the most pressing issues in these communities. We used this approach to enhance the effectiveness and efficiency of the chatbot. Our team has aimed to bridge the gap between technological innovation and real-world application by adopting bottom-up co-development methods. This, in turn, would lead to sustainable and impactful advancement in community health.
Authored by Sreya Majumdar, Ankita Sharma and Neelanjana Das
The author(s) would like to thank Dr. D Praveen, Prof. Jane Hirst, Dr Huiqi Yvonne Lu, Yasmina Al Ghadban, Uday Adavi and Sridevi Gara for their invaluable support and contributions throughout the development of this blog.
References
1. Process evaluation of the SHP2 intervention is currently being conducted. Findings from the initial round of qualitative interviews with ASHAs, Auxiliary Nurse Midwives (ANMs), PHC doctors, and women has highlighted several perceived benefits of the intervention. These include the provision of home visits for women, free diagnostic tests with immediate results, and improved accuracy of test records.
2. ASHAs were grouped as younger and older based on their age and experience as ASHAs.
Share this Post
Stay connected and updated
Subscribe to our mailing list for the latest news, events, and updates in health research.