Exploring social accountability for indigenous and marginalised communities by exchanging experiences from Brazil, India, Mozambique and other parts of the world
A satellite session of the Health Equity Network India at the COPASAH Global Symposium 2019.
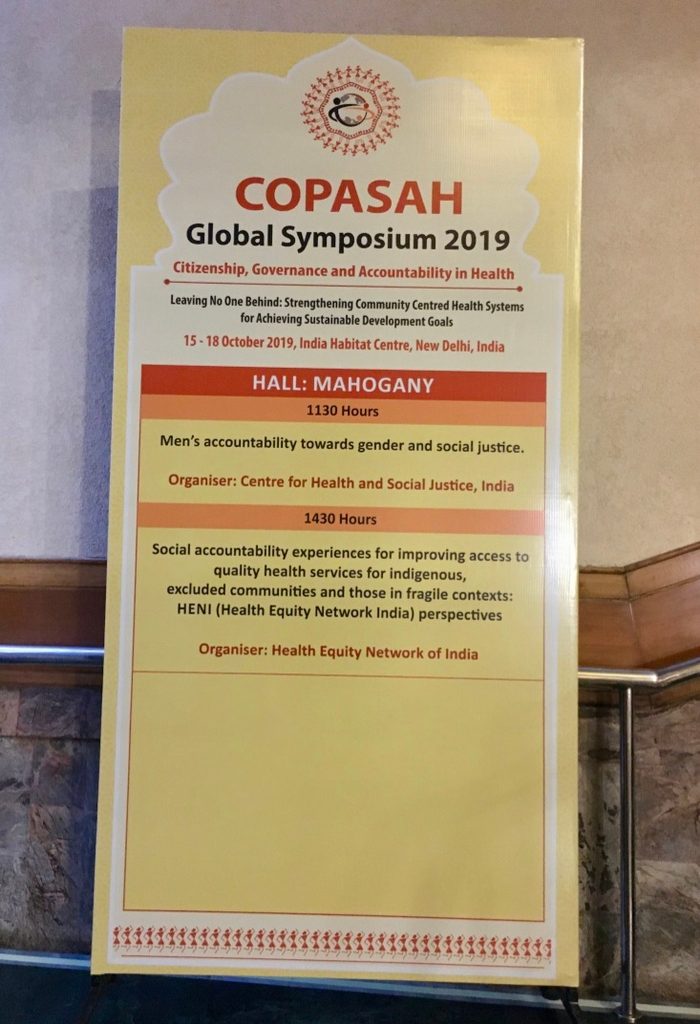
In mid-October, the Global Symposium for COPASAH 2019 organised a day of satellite sessions prior to the symposium launch on 15 October 2019. The Health Equity Network India or HENI organised a workshop as a satellite session titled ‘Social accountability experiences for improving access to quality health services for indigenous, excluded communities & those in fragile contexts: HENI (Health Equity Network India) perspectives’.
This workshop aimed to share different experiences of mobilising indigenous communities around social determinants of health inequities and to then draw on those experiences to develop an in-depth understanding of social accountability towards these communities and think of effective strategies for the same.
To achieve this, HENI brought together speakers from Brazil, Mozambique and different parts of India to share their experiences working with/for indigenous communities. These speakers included:
- C Mahadeva from the Zilla Budakkattu Girijana Abhivrudhhi Sangha and Community Researcher at The George Institute of Global Health India (Karnataka, India) spoke on forest rights and health by providing a brief overview of the struggles of his people (the Soliga people) in southern Karnataka
- Danilo Paiva Ramos from the Universidade Federal da Bahia and Brazilian Health Unlimited (Brazil) spoke about the Brazilian indigenous social movement's strategies to improve accountability and governance in health
- Vandana Prasad from the Public Health Resource Network (Jharkhand, India) challenged some assumptions of mainstream programmes to achieve health and nutrition outcomes for tribal communities, based on the experiences of her work
- Eduarado Malo from Namati (Mozambique) spoke about their experience of making village health committees a regular, potent force for the local health accountability across the country using a legal framework
- Julee Jerang from the Institute of Public Health Bengaluru (Arunachal Pradesh, India) shared her findings and reflections as a researcher from a comparative study on health outcomes and socio-economic status between Scheduled and non-Scheduled Tribes’ population around forest in north-east India
After listening to these experiences, the participants were divided into three groups and discussed around four questions,
a) how do we understand indigenous health,
b) what does accountability mean for indigenous health,
c) strategies used around indigenous health through case studies and participants’ experiences, and
d) lessons learnt.
The workshop had 42 participants even though the room could only seat about 30, and the participants came from different states of India and other countries like Peru, Brazil, Mozambique, Uganda, Guatemala and United Kingdom. The experiences around the room were also diverse and rich with a mix of academicians, researchers and activists who worked with indigenous people in their own regions. This made for vibrant and engaging group discussions in the second half of the session.
The session closed with sharing of key points addressing the questions posed to the groups by a representative from each and summarised by Renu Khanna, Steering Group member of HENI. Some of the recurring themes were about the lack and hence need for political will for indigenous health, the need to recognise and find ways to address the global and transnational forces that influence local health systems, to move away from a ‘one size fits all’ model towards bringing in more people’s voice in participation and responsive communication and the importance of collectivisation not just for building solidarity in the community but also across stakeholders. Other important points identified in building our understanding of social accountability of indigenous people were not homogenising these communities, recognising their concept of health and also that accountability for health meant accountability for the wider determinants for better wellbeing and not just for health services.
For C Mahadeva, this was a unique experience. As a community leader and the President of the Zilla Budakkattu Girijana Abhivrudhhi Sangha (district-level community based organisation of indigenous peoples) in Chamarajanagar district, he had participated in events at different levels from grassroots to national level. However this was his first experience speaking and interacting with an international audience, and as a community researcher, his first interaction with researchers and activists who worked with indigenous peoples from across the world.
He presented his talk on the struggles for forest rights of his people in Kannada but followed the conversations in English and even interacted one-on-one with international researchers and activists during the breaks and after the workshop. He was humbled on one hand to find out that his people’s struggles with forest rights was widely appreciated and recognised as an experience that others could learn from. On the other hand, he also recognised the common threads that emerged from varied experiences across the globe like distinct socio-cultural identities and political histories of indigenous communities and their influence on their health status and access to health services today.
In the end, he also identified the difference of wearing a researcher hat than that of a community leader, and was thankful to the different perspective he had gained through his work with TGI’s implementation research study on community health workers working with his people.
To know more about the experiences of the Soliga people, please contact C Mahadeva or Tanya Seshadri. To find out more about the Health Equity Network India, please contact the HENI Coordinator.
Related people

Photo Gallery